Sternocleidomastoideus: Neck Flexors
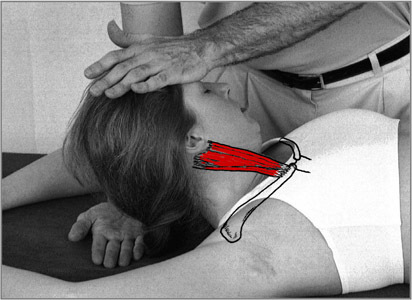
Origin: Sternal head: on the anterior surface of the manubrium (top-front of the sternum).
Clavicular head: upon the upper surface of the medial half of the clavicle.
Insertion: Upon the lateral surface of the mastoid process and the superior nuchal line of the occiput.
Action: One-sided contraction pulls the head toward the shoulder on the same side as the muscle and rotates the head toward the opposite side. Bilateral contraction flexes the head upon the neck.
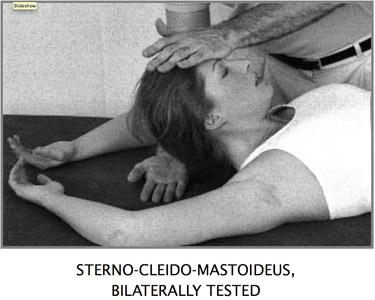
Position: The patient lies upon the back. The arms are flexed and lifted above the head to avoid pressing on the table during the test. To test bilaterally, the patient flexes (lifts) the head from the table. To test unilaterally, the patient fully rotates the head away from the side to be tested and lifts it from the table. The examiner places his other hand upon the table under the head to catch it in case of weakness.
Stabilization: Tested supine, the table provides the necessary stabilization. If this test is performed standing, the examiner must provide stabilization with one hand upon the upper back. When testing in this position, as soon as the muscle demonstrates any weakness, the test pressure must immediately cease. Great care must be observed to never push the head back and down, which could damage the neck.
Muscle Test, Bilateral: Using a broad area of con- tact, the examiner places his hand upon the middle of the forehead of the patient and presses posterior, carefully following the arc of the anatomical movement. Under no conditions should the pressure be straight down toward the table, which could injure the intervertebral discs. In the unilateral test, the examiner places his hand upon the parietal bone. The exact area of contact is defined by how far the patient can rotate his head. The direction of pressure is posterior and slightly lateral, in a curve following the anatomical arc of motion produced by the contraction of the muscle.
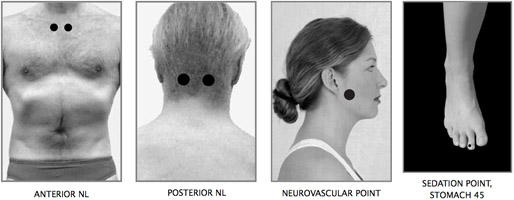
Front Neurolymphatic: 1st intercostal space, about 9 cm from the sternum.
Back Neurolymphatic: C2 lamina.
Neurovascular: Ramus of the jaw below the zygoma.
Reactive Muscles: Neck extensors, upper trapezius, pectoralis major clavicularis, opposite sternocleidomastoideus.
Meridian: Stomach.
Organ: Sinuses, lymphatic drainage of the head.
Nutrition: B6, B3 (niacinamide or niacin), organic iodine, herbal and homeopathic remedies for the sinuses, especially nosodes and lymph drainage remedies. Leaf recommends a 5-to-1 ratio of niacinamide or niacin to B6 as being most effective.
Discussion: The sternocleidomastoideus (SCM) is actually a group of several associated muscles. The contraction of the sterno-cleido-mastoideus is easily visible, springing out of the neck during the muscle test. Although quite useful as a general test, the bilateral test does not adequately isolate the SCM. In this test, the scalenes and several other neck flexor muscles are also active. To best isolate the SCM, the head should be maximally rotated, and the SCM of each side tested independently. The examiner observes for any attempt to reduce the angle of rotation during the test. This usually indicates a weakness of the SCM and an attempt to recruit the scalenes, which are most active at 10° of rotation. Inability to remain in the full rotation or pain upon doing so should be considered a sign of muscle weakness and treated without put- ting the patient into unnecessary stress or pain that could be caused by testing. Pressure is applied in the direction of the tangent of the arc produced by the anatomical motion of contraction of the SCM. Apply- ing test pressure with a broad contact of the palm avoids possible tugging on the skin, which can pro- duce a false weakness of the muscle test.
Patients with chronic sinus conditions or problems in the upper vertebrae of the neck may have extremely weak-testing neck flexors. In such cases, this test is only to be performed with very gentle test pressure.
The neck flexors are functionally much weaker than their opponents, the neck extensors. Due in part to the postural habit of holding the head far forward of the line of gravity, the neck extensors rarely relax. This often creates a pattern of (chronically tight) primary muscle-neck extensors to (chronically weak, inhibited) reactive muscle-neck flexors. If this condition exists, treatments to strengthen the neck flexors will only have temporary success until the treatment for reactive muscles is applied. To test for such reactivity, the neck flexors must first test strong or be temporarily strengthened, for example, by massage of the appropriate neurolymphatic reflex points. Then the neck extensors are contracted bilaterally. If the patient is supine, this may be easily accomplished by having the patient firmly pull the head back down upon the table.
Immediately following this contraction of the neck extensors, the neck flexors are bilaterally tested. If they now test weak, treatment for reactive muscles is indicated. In this case, such treatment consists of neuromuscular spindle cell pinching of the belly on the upper trapezius muscles and other neck extensors located parallel to the spine in the neck, parallel to the contracting length of the muscles. Areas of palpable hardness are repeatedly and deeply pinched. Support must be given to the forehead so the neck extensors are not contracted against the force required for the neuromuscular spindle cell pinching treatment. This may be accomplished by having the patient sit next to the table, place his elbows upon the table, and his forehead upon the heels of his hands. Alternatively, he can lie prone with his forehead upon his forearm or a hard pillow. It is important to pinch deeply into the muscle and not only upon the skin. Then the neck muscles are tested bilaterally to reset them. This process is repeated several times, focusing upon the areas of hardness and/or pain in the upper trapezius muscles and other neck extensors. After effective treatment, contraction of the neck extensors should no longer weaken the neck flexors.
Reactive conditions may also exist between unilateral SCM and upper trapezius muscles and also between the SCM muscles on each side. A noteworthy reactive condition may also be observed between the reactive SCM on one side and the contralateral psoas muscle. The author observed and treated this condition in a European soccer player. After hitting the ball very hard with one side of his head, he found that the SCM on that side became hypertonic. Subsequently, the insertion of the psoas on the opposite side of his body became extremely tender to the touch and painful when he stood or ran. Not only was the contralateral psoas insertion tender, it also tested weak on this side. The inhibition of the contralateral psoas muscle, created by the hypertonic SCM, also caused him to be out of balance and unstable when upright. Reactive muscle treatment directed toward the hypertonic SCM eliminated the pain and improved his balance and coordination.
Notice in this case how the activity of the unilateral SCM nearly mirrors the activity of the contralateral psoas. The contraction of the right SCM pulls the head forward and pulls the right ear toward the midline. The contraction of the left psoas lifts the left leg forward and pulls it toward the midline. Though the whole trunk lies between them, so considered, these two muscles may be seen as having a related and opposing function. This is an example of the complex relationship often observed between muscle pairs involved in reactive conditions.
Reactive muscle treatment should be long lasting. However, the postural problem that caused the chronic contraction of the neck extensors needs to be corrected, for example, by lessons in Alexander Technique (training in optimal posture and movement of the body). Or, if the cause of the muscular imbalance was a trauma, emotional stress release methods may need to be performed. If these steps are skipped and the reactivity is only treated manually, the reactive condition with the associated patterns of tension, pain and possible malfunction of the gait mechanism is likely to recur.
Malfunction of the neck flexors often causes peripheral nerve and vascular entrapments in the shoulders and arms. When this is suspected, have the patient lie supine and test the function of various arm muscles that should test strong. Then retest the same muscles with the head elevated and rotated to contract the neck flexors. If the muscles now test weak, have the patient expand and lift the rib cage. If this does not cause a strengthening of the formerly weak- testing muscles, a nerve entrapment has been located. These may be corrected with AK procedures such as chill and stretch or fascial release, carefully applied to the SCM.
The SCM is particularly interesting because it has double enervation from C2–C3 and from the tenth cranial nerve. The only other muscle in the body that has double enervation is the upper trapezius, which is the major neck extensor. These two muscles have a finely attuned simultaneous interaction without which the fine coordination of the walking (gait) pat- tern would not be possible. Goodheart suggests that the double enervation of these muscles is necessary for the correct function of the gait coordination. In walking or running, there should be a well-orchestrated facilitation and inhibition of the next flexors and extensors. When the left leg steps forward, the right shoulder moves forward. In order to keep the head facing forward, the right SCM as well as the left upper trapezius (and other left neck extensors) are inhibited. This is the normal walking or gait coordination. Goodheart devised a method to test for the normal facilitation and inhibition of these muscles:
The patient steps forward on his right foot and puts much of his weight upon it. Some weight is also upon the ball of the left foot with the heel raised as would be the case when taking a step in walking. In this position, the SCM and upper trapezius muscles are tested. If the gait mechanism is intact, in this position the left SCM and the right upper trapezius should be inhibited and therefore test weak. Since the upper trapezius is typically in a state of chronic tension, the weakness produced in this test may be difficult to ascertain.
Unilateral weakness of the SCM and/or upper trapezius muscles can produce a lateral tilt of the head, which may cause occipital or upper cervical subluxation and improper stimulation of the head-on-neck reflexes, with consequent disruption of the equilibrium mechanism. In cases of dizziness, this possible cause should be considered.
In my work as a psychologist, I have observed that bilateral weakness of the neck flexors is often coupled with a weakened ability to effectively overcome obstacles and push one’s will through against the opposition of others. These muscles must be strong in order to “butt heads” effectively, as observed in dominance rituals in the animal kingdom. Weak-testing neck flexors may be associated with being a “pushover.” These are only anecdotal observations and do not (yet) form an official part of Applied Kinesiology.